54Y/M with vomitings fever and sob
THIS IS AN ONLINE E LOG BOOK TO DISCUSS OUR PATIENT'S DE - IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS / HER /GUARDIAN'S SIGNED INFORMED CONSENT .HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH SERIES OF INPUTS FROM AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS WITH AN AIM TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE BASED INPUT.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
November 26
Chief complaints :
C/o fever since 5 days
C/o sob since 5 days
C/o vomiting since 3 days
History of presenting illness :
Patient was apparently asymtomatic 5 days then had fever since 5 days which is of high grade , associated with chills and not relieved on taking medication
He complaints of shortness of breath since 5 which is grade 2 ( MMRC)
No orthopnea and paroxysmal nocturnal dysnea is present
He also complaints of vomiting since 3 days , 2-3 episodes per day which is non bilious non projectile and watery content
There was an ulcer over left foot since 1 month which is associated with edema of foot and there is sudden onset of bleb since yesterday
HISTORY OF PAST ILLNESS
K/C/O DM type 2 since 14 years and is on medication
Metformin 500 mg and Glimepiride 1 mg
K/C/O Hypertension since 10 years and is on medication Amlodipine 5 mg




PERSONAL HISTORY :
Pt is vegetarian since childhood
Appetite - decreased
Sleep - adequate
Bowel and bladder movements - regular
No known allergies
No addictions
FAMILY HISTORY
Both of his parents had diabetes
Father is on medication
GENERAL EXAMINATION
Patient was conscious coherent and cooperative
No pallor icterus clubbing cyanosis generalized lymadenopathy
Edema is present in left foot upto the ankle
VITALS
BP - 80/60mmhg
PR - 104bpm
RR - 18 cpm
Systemic examination
CVS - S1s2 heard no murmurs
RR - normal vesicular breath sounds
PA - soft and non tender and no organomegaly
CNS - no focal neurological deficit
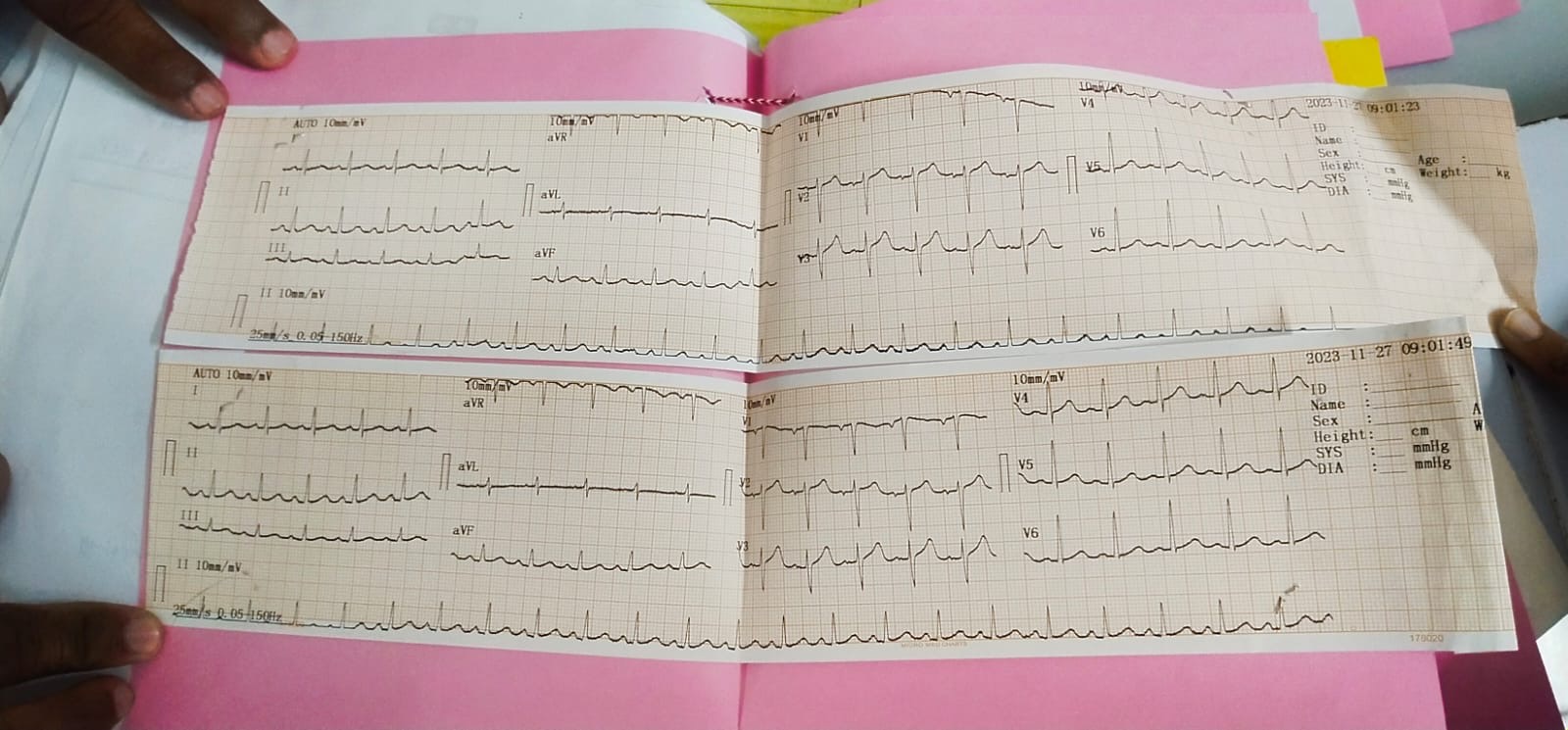
INVESTIGATION
RBS - 311mg/dl





TYPE 2 Diabetes mellitus
Left diabetic foot and HYPERTENSION
TREATMENT
1) IV fluids NS 100ml/hr
2) INJ H. ACTRAPID Sc / TID ( acc to GRBS info )
3) GRBS monitoring
4 ) BP monitoring hourly
28/11/2023
O/E
PR 92bpm
BP 140/90
RR 26cpm
GRBS 157mg/dl
CVS - s1s2 heard no murmurs
PA - soft non tender
RR - nvbs
CNS - no focal neurological deficit
FBS
PLBS - 178 mg/dl
Rx :
1) iv fluids 75ml / hr
2) inj AUGUMENTIN 1.2g IV/BD ( 9am ; 8 pm )
3 ) inj PIPTAZ 4.5g TID (8am , 1pm ,8pm )
4 )T linezolid 600mg BD
5) inj H ACTRAPID SC TID ( 6u;6u;6u )
6 ) inj NPh sc bd ( 4u ;4u )
7) T LASIX 40 mg bd
8) T ecospirin 75 mg OD
9) GRBs
10 ) temp monitoring 4 hrly
11) T AMLODIPINE 5mg OD
12 ) T CHYMORAL FORTE bd
13) T CILASTOL 100 mg BD
14) T ATORVASTATIN 40 mg OD


Comments
Post a Comment