A case of CKD
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.”
A 64 yr old male who is a resident of nalgonda farmer by occupation came to the opd with the chief complaint of NO URINATION SINCE 3 days .
HISTORY OF PRESENTING ILLNESS
Patient was apparently asymptomatic 4 years back
Later He developed PAIN ABDOMEN and TIGHTNESS
and came to hospital for which he was diagnosed as having RENAL CALICULI and underwent Percutaneous nephrostomy
in our hospital and later discharged . Later he developed GENERALISED WEAKNESS and DIZZINESS for which he was diagnosed as DIABETES MELLITUS TYPE 2 and HYPERTENSION 2 years ago. On irregular medication 2 yrs back ( 2020 Nov ) on being unresponsive and was in ICU for 4-5 days and diagnosed to be hypoglycaemic and creatinine is 5.94 , denied for dialysis and discharged. Pedal edema was on and off and no decreased urine output , no hematuria .
Fever associated with loose stools 10 days back , with decreased urine output for 1 day and anuria for 3 days taken to the hospital and underwent 4 sessions of hemodialysis and came here for hemodialysis .


PAST HISTORY
2 years ago he was diagnosed as having RENAL CALICULI and underwent PCN .
K/C/O Diabetes mellitus since 2 years
K/C/O Hypertension since 2 years
N/K/C/O Asthma , Tuberculosis , epilepsy
PERSONAL HISTORY
Appetite - lost
Eggetarian
He has diarrhoea
Micturition - abnormal ( Anuria )
HABITS
Alcohol- occasionally
Tobacco - smoking chutta
GENERAL EXAMINATION
Pallor - Present
Icterus - absent
Cyanosis- absent
Clubbing- absent
Lymphadenopathy- absent
Edema - present ( Anasarca )

VITALS :
Temperature – 101°F
Pulse rate –106 per min
BP –160/90
Respiration rate –
GRBS – 177mg %
SPO - 96 percent
GRBS - 177mg%
SYSTEMIC EXAMINATION
CVS
No Thrills
Cardiac sounds S1,S2+
No murmurs
RESPIRATORY SYSTEM
Dyspnoea - present
Wheeze - absent
Position of trachea - central
Breath sounds are vesicular
ABDOMINAL EXAMINATION
Abdomen is obese
No Tenderness
No palpable mass
Hernial orifices normal
No free fluid
No bruits
Liver is not palpable
Spleen is not palpable
Bowel sounds heard
CNS
Conscious
Speech is normal
Signs of meningeal irritation- no neck stiffness
Kernings sign negative
Cerebral signs - No finger nose in coordination
No knee-heel in coordination
PROVISIONAL DIAGNOSIS
Chronic renal failure with
T2 DM and HTN
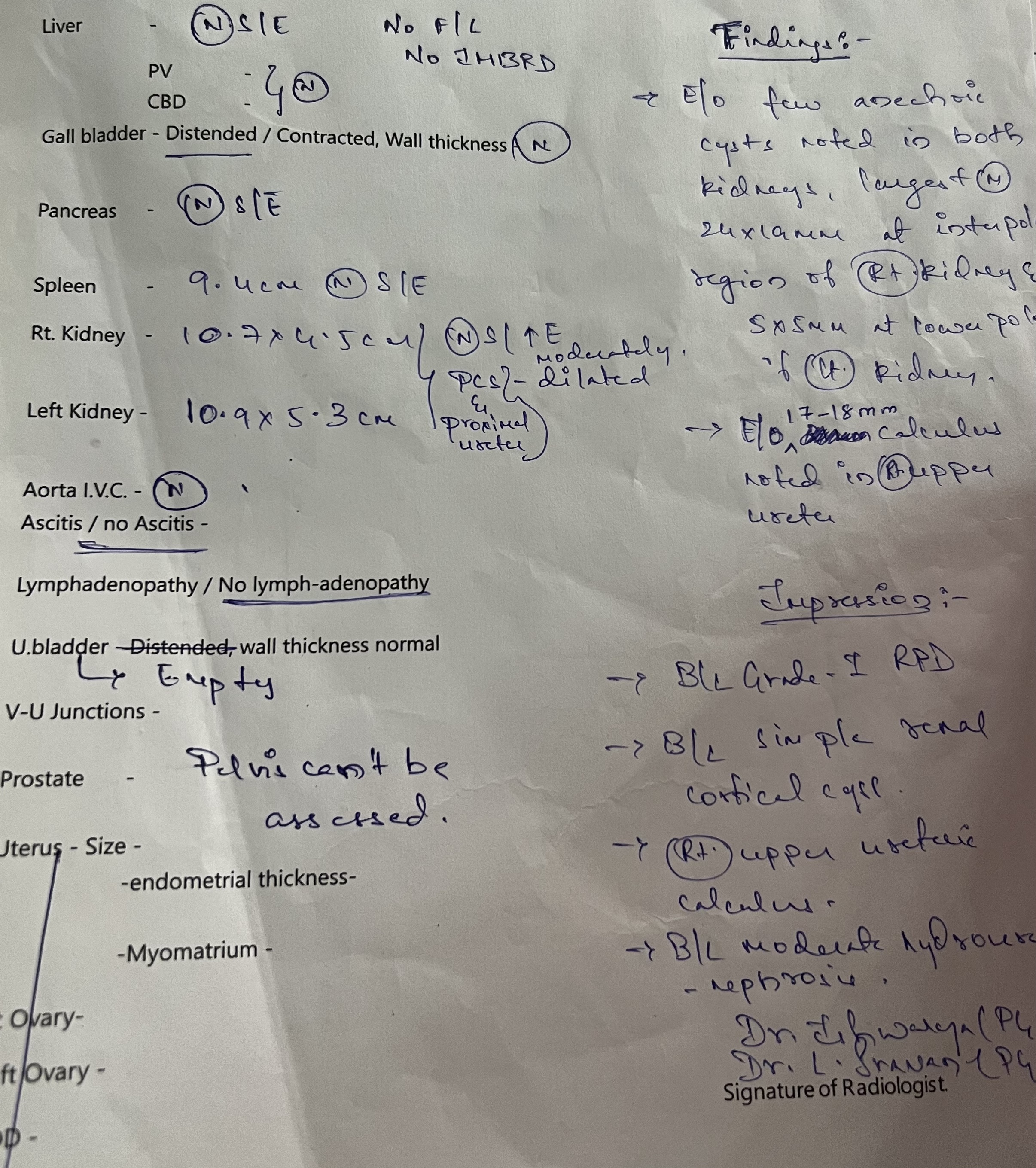
Investigations


ULTRASOUND







TREATMENT
1)salt restriction< 1 to 2 gm/day
2)fluid restriction < 2L/day
3) inj LASIX 40 mg IV BD
4) tab .NICARDIA 10mg PO BD
5)tab.NODOSIS 500mg PO BD
6)tab. SHELCAL 500Mg PO OD
7)tab. OROFER-XT PO OD
8)inj.erythropoetin 4000IU
9) haemodialysis ,
Antibiotics after culture
on 5/7/22
BP: 100/70 mm of Hg
PR:77 bpm
RS: 18 Cpm
CVS : SI and S2 Normal
CNS: NAD
per abdomen: soft and non tender
6/7/22
BP:90/60 Mm Hg
PR:86 bpm
C VS:SI,S2 +
C NS :NAD
per abdomen:softand non tender
Treatment
Inj Lasix40mg IV Bd
Tab. Nicardia
T. Nodosis
T. Shelcal
T. Orofor
T. Dolo
7/7 / 22
BP:110/60 mm Hg
PR:80 bpm
C V S :SI,S2 +
CN S:NAD
per abdomen:soft and nontender
Treatment
Inj Lasix
Tab. Nicardia
T. Nodosis
T. Shelcal
T. Orofer
T.Dolo


Comments
Post a Comment